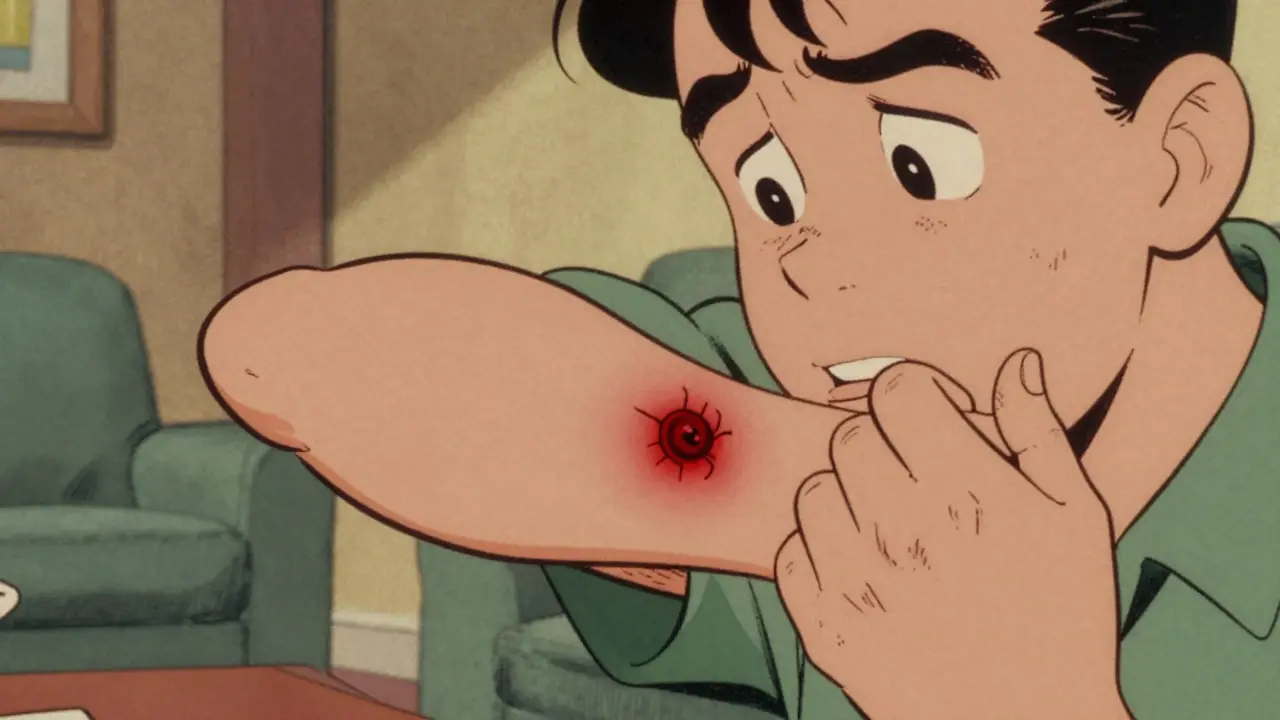
It starts as a small red bump on your leg or arm. You might mistake it for a spider bite or a simple pimple. But within days, it swells, becomes painful, and fills with pus. This is not just a minor skin irritation; it could be Methicillin-Resistant Staphylococcus aureus, commonly known as MRSA. It is a strain of bacteria that has evolved to resist many common antibiotics, making infections harder to treat and more dangerous than typical staph infections. For decades, doctors believed MRSA was strictly a hospital problem. Today, that line has blurred significantly. Understanding where you caught it-and which type of bacteria you are fighting-is the difference between a quick recovery and a life-threatening complication.
The Two Faces of MRSA: Community vs. Hospital
To understand how to fight MRSA, you first need to know what you are up against. The bacteria Staphylococcus aureus lives harmlessly on the skin or in the nose of about one-third of all people. However, some strains have developed a genetic defense mechanism called the mecA gene, which allows them to survive exposure to beta-lactam antibiotics like methicillin, penicillin, and amoxicillin. These resistant strains are classified into two main categories based on where they typically spread and their genetic makeup: Community-Associated MRSA (CA-MRSA) and Healthcare-Associated MRSA (HA-MRSA).
Community-Associated MRSA (CA-MRSA) emerged in the late 1990s among healthy individuals with no recent hospital stays. According to data from the Centers for Disease Control and Prevention (CDC), CA-MRSA accounts for a significant portion of invasive infections in otherwise healthy people. The dominant strain in the United States is USA300, a highly virulent clone responsible for approximately 70% of CA-MRSA cases. This strain is notorious for producing toxins like Panton-Valentine leukocidin (PVL), which destroys white blood cells and causes severe tissue damage. If you play contact sports, live in crowded housing, or share personal items like towels, you are at higher risk for this type.
Healthcare-Associated MRSA (HA-MRSA), on the other hand, thrives in medical settings. It affects patients who have been hospitalized, undergone surgery, had dialysis, or have indwelling devices like catheters. HA-MRSA strains are genetically different; they often carry larger resistance genes (SCCmec types I-III) that make them impervious to a wide range of antibiotics, including erythromycin, clindamycin, and fluoroquinolones. While CA-MRSA is aggressive and fast-acting, HA-MRSA is stubborn and hard to kill due to its extensive drug resistance profile.
| Feature | Community-Associated (CA-MRSA) | Healthcare-Associated (HA-MRSA) |
|---|---|---|
| Patient Profile | Healthy individuals, athletes, military personnel | Hospitalized patients, elderly, immunocompromised |
| Dominant Strain | USA300 | ST239, ST5 (varies by region) |
| Virulence Factors | High production of PVL toxin | Lower PVL production, higher resistance genes |
| Antibiotic Resistance | Often susceptible to clindamycin, TMP-SMX | Multi-drug resistant (erythromycin, clindamycin, etc.) |
| Typical Infection Site | Skin and soft tissue abscesses | Bloodstream, surgical sites, lungs |
How MRSA Spreads: The Blurring Lines
In the past, infection control protocols treated hospitals and communities as separate ecosystems. That strategy is failing. Research published in PLOS Pathogens highlights that the distinction between CA-MRSA and HA-MRSA is increasingly meaningless in practice. We now see bidirectional transmission: community strains entering hospitals, and hospital strains leaking back into the community.
Consider the numbers: A study in Alberta, Canada, found that nearly 28% of hospital-onset MRSA infections were caused by community-type strains. Conversely, over 27% of community-associated infections were driven by hospital-type strains. How does this happen? It comes down to human movement and survival time. An average hospital stay lasts only four to five days, but MRSA can colonize a person’s nose or skin for hundreds of days. When a patient goes home after surgery, they may carry HA-MRSA with them. When a healthy person with CA-MRSA gets injured and seeks emergency care, they bring the virus into the sterile environment of the hospital.
Certain environments act as super-spreaders for CA-MRSA. Crowded living conditions facilitate rapid transmission through skin-to-skin contact and shared surfaces. Data shows significantly elevated risks in specific settings:
- Prisons: Up to 14.9 times higher risk due to close quarters and limited hygiene resources.
- Military Barracks: 12.3 times higher risk because of intense physical contact during training and shared equipment.
- Homeless Shelters: 8.7 times higher risk linked to poor sanitation and wound exposure.
- Subsidized Housing: 6.2 times higher risk associated with overcrowding.
Another major reservoir is among people who inject drugs. The reuse of needles and poor injection site hygiene allow strains like USA300 to thrive and spread rapidly within these networks before moving into the general population.
Recognizing the Symptoms Early
Early detection is critical because MRSA can escalate from a skin nuisance to a systemic threat quickly. Most CA-MRSA infections present as skin and soft tissue issues. Look for these warning signs:
- A red, swollen, and painful lump under the skin.
- An area that feels warm to the touch.
- Pus or fluid draining from the center of the lesion.
- Fever accompanying the skin infection.
If the bacteria enter the bloodstream-a condition known as bacteremia-the symptoms become severe and life-threatening. You might experience chills, low blood pressure, confusion, or difficulty breathing. HA-MRSA is more likely to cause these deep-seated infections, such as pneumonia following intubation or infections at surgical incision sites. Unlike CA-MRSA, which often stays localized to the skin, HA-MRSA frequently invades deeper tissues and organs.
Treatment Strategies: What Works?
Treating MRSA requires precision. Because standard antibiotics like amoxicillin fail against MRSA, doctors must choose alternative medications based on the suspected strain and severity of the infection. The approach differs drastically between mild skin infections and serious invasive diseases.
For Mild Skin Infections (CA-MRSA): Often, the most effective treatment is mechanical rather than chemical. Incision and drainage (I&D) alone can cure many small abscesses without any antibiotics. If medication is needed, oral antibiotics with high susceptibility rates are preferred. Studies show that Clindamycin remains effective against 96% of CA-MRSA isolates. Other reliable options include Trimethoprim-sulfamethoxazole (TMP-SMX) (92% susceptibility) and tetracyclines like doxycycline (89% susceptibility). These drugs are affordable, widely available, and generally well-tolerated.
For Severe or Hospital-Acquired Infections (HA-MRSA): When MRSA enters the blood or lungs, or when the strain is multi-drug resistant, stronger intravenous (IV) antibiotics are necessary. Vancomycin has long been the gold standard for treating HA-MRSA. However, rising resistance to vancomycin has led clinicians to use alternatives like Daptomycin, which disrupts bacterial cell membranes, or Linezolid, which inhibits protein synthesis. These drugs are powerful but come with higher costs and potential side effects, such as muscle toxicity or nerve damage, requiring careful monitoring.
A growing challenge is the emergence of "hybrid" strains. These bacteria combine the high virulence of CA-MRSA with the broad antibiotic resistance of HA-MRSA. This makes empirical treatment-guessing the right drug before lab results return-increasingly difficult. Doctors are now urged to obtain cultures immediately to guide therapy, rather than relying on historical assumptions about where the infection came from.

Prevention: Breaking the Chain of Transmission
Since antibiotics are losing the battle against evolving bacteria, prevention is our strongest weapon. The goal is to stop colonization and transmission before an infection takes hold. Here are evidence-based steps to protect yourself and others:
- Hand Hygiene: Wash hands frequently with soap and water for at least 20 seconds. Alcohol-based hand sanitizers are also effective against MRSA. This is the single most important step in preventing spread.
- Wound Care: Keep cuts and scrapes clean and covered with a dry, sterile bandage until fully healed. Do not share razors, towels, or athletic gear that touches open skin.
- Environmental Cleaning: Regularly disinfect high-touch surfaces like doorknobs, gym equipment, and bathroom fixtures. Bleach-based cleaners are particularly effective against MRSA spores.
- Decolonization Protocols: For recurrent carriers, doctors may prescribe mupirocin ointment for the nose and chlorhexidine body wash. This reduces the bacterial load on the skin and in the nasal passages, lowering the risk of self-infection and transmission to others.
- Avoid Unnecessary Antibiotics: Overuse of antibiotics drives resistance. Only take antibiotics when prescribed for bacterial infections, and always finish the full course. Never share leftover pills.
Hospitals are also adapting. Traditional isolation measures are being supplemented with active surveillance-swabbing patients upon admission to detect MRSA carriage early. Contact precautions, including gloves and gowns, remain essential for staff caring for infected patients. However, experts argue that we need integrated surveillance systems that track MRSA across both healthcare and community settings to truly curb its spread.
The Future of MRSA Management
The landscape of infectious disease is shifting. As community reservoirs expand, the old model of treating hospital and community MRSA as separate entities is obsolete. Mathematical models suggest that without intervention, highly transmissible community strains could eventually dominate hospital settings, overwhelming current control measures.
We are seeing new clones emerge globally. In China, for example, the ST59 strain is becoming a common HA-MRSA clone alongside the traditional ST239. This evolution demands constant vigilance and updated guidelines. Public health agencies must focus on education, ensuring that athletes, parents, and healthcare workers understand the risks and preventive measures.
Ultimately, managing MRSA requires a collective effort. From proper hygiene in locker rooms to strict protocols in intensive care units, every break in the chain of transmission saves lives. By recognizing the symptoms early, seeking appropriate treatment, and practicing rigorous prevention, we can stay ahead of this resilient superbug.
What is the difference between CA-MRSA and HA-MRSA?
CA-MRSA (Community-Associated) typically infects healthy people outside of healthcare settings and is often caused by the USA300 strain, which produces toxins causing severe skin infections. HA-MRSA (Healthcare-Associated) affects patients in hospitals or clinics and is usually more resistant to multiple classes of antibiotics, making it harder to treat. However, the lines are blurring, with strains moving between both environments.
How long does it take to recover from an MRSA infection?
Recovery time depends on the severity and location of the infection. Simple skin abscesses treated with incision and drainage may heal within a week. More severe infections requiring IV antibiotics, such as those affecting the blood or lungs, can take several weeks to resolve. Patients with HA-MRSA often have longer hospital stays, averaging 13 to 21 days, compared to 1.5 to 2.8 days for CA-MRSA skin infections.
Can you get MRSA from a pet?
While rare, it is possible for MRSA to transmit between humans and animals, including pets like dogs and cats. Pets can become colonized or infected if they have close contact with an infected human. If you have an MRSA infection, avoid letting your pets lick your wounds, and consult a veterinarian if your pet develops similar skin lesions.
Is MRSA contagious?
Yes, MRSA is contagious. It spreads through direct skin-to-skin contact with an infected person or carrier, or by touching contaminated objects like towels, razors, or gym equipment. People who are colonized with MRSA (carrying it in their nose or on their skin without symptoms) can still spread it to others, especially if they have open wounds or weakened immune systems.
What are the best antibiotics for treating MRSA?
For mild CA-MRSA skin infections, oral antibiotics like clindamycin, trimethoprim-sulfamethoxazole (TMP-SMX), or doxycycline are often effective. For severe or HA-MRSA infections, intravenous antibiotics such as vancomycin, daptomycin, or linezolid are required. The choice of antibiotic should always be guided by culture and sensitivity testing to ensure the specific strain is susceptible to the chosen drug.




Comments
Great breakdown of the USA300 strain dynamics. I work in infectious disease control and seeing the shift from HA-MRSA to CA-MRSA dominance has been wild. The part about incision and drainage being sufficient for small abscesses is crucial because patients often panic and demand antibiotics immediately. We have to educate them that mechanical removal is often the cure, not just chemical warfare against the bacteria. It saves on resistance buildup too.
This article is full of western bias. In India we deal with superbugs daily but nobody writes these fancy articles about it. Your hospitals are dirty and you blame the community. We have better hygiene protocols in our crowded cities than your sterile labs. Stop pretending you understand global health when you only look at US data. It is insulting to those who actually live with this reality every single day without your expensive drugs.
actually the distinction between CA and HA is becoming irrelevant which is why the blurring lines section is so important 🧬 most people here dont read past the title. the real issue is that we treat symptoms not causes. also bleach doesnt kill spores it kills vegetative cells so that advice is slightly off unless you mean specific formulations. interesting read though 👏
I must say, the table comparing virulence factors was exceptionally clear. It is fascinating how the PVL toxin specifically targets white blood cells, creating that necrotic appearance we see in severe cases. One might argue that the environmental cleaning section should emphasize contact time more heavily, as many commercial disinfectants require ten minutes of wet contact to be truly effective against staphylococci. Thank you for sharing this comprehensive overview; it is a valuable resource for anyone concerned about skin health.
omg i had this last year and thought it was just a spider bite until my whole leg swelled up 😱 thank god i went to the er quickly. the doc said it was ca-mrsa and just cut it open and let it drain. no pills needed! i feel like people are so scared of antibiotics they forget about basic wound care. keep your cuts covered ppl!! its scary stuff but manageable if you act fast 💪✨
u guys are missing the point. its not about the bug its about the system. hospitals are profit centers not healing places. they push vancomycin because its expensive not because its best. i know a nurse who says they isolate patients too late. its negligence plain and simple. stop blaming athletes and start blaming the admins who cut corners on cleaning staff wages. its disgusting really.
The moral decay of society is reflected in our microbiome. We share what should remain private. The boundary of the self is dissolving. MRSA is merely a symptom of our collective failure to maintain individual sanctity. Hygiene is not just physical; it is spiritual. You cannot sanitize the soul with bleach. This article treats the leaf, not the root. The root is our lack of discipline.
I appreciate everyone sharing their perspectives here. It is really helpful to hear from both medical professionals and those who have experienced infections firsthand. The variety of viewpoints helps paint a complete picture of how complex MRSA transmission can be in different settings. Let us all stay informed and take care of each other by practicing good hygiene and supporting public health initiatives. It is a team effort!