Imagine a silent pressure building inside your abdomen, pushing against veins that were never meant to carry that much blood. For people with advanced liver disease, this isn't just discomfort-it's a ticking time bomb. Variceal bleeding is a life-threatening gastrointestinal emergency caused by ruptured veins in the esophagus or stomach due to portal hypertension. When these swollen veins burst, the situation becomes critical fast. Mortality rates hover between 15% and 20% within the first six weeks if not managed aggressively. But here is the good news: modern medicine has developed highly effective strategies to stop the bleeding, prevent it from coming back, and keep you alive. This guide breaks down exactly how banding, beta-blockers, and prevention work together to save lives.
Understanding the Pressure: Why Varices Bleed
To understand why treatment works, you first need to understand the problem. In a healthy body, blood flows smoothly through the liver. But when scarring from liver cirrhosis blocks normal flow, pressure builds up in the portal vein system. This condition is called portal hypertension. Think of it like a traffic jam on a highway; when the main route is blocked, cars (blood) try to squeeze through smaller side streets. These "side streets" are the collateral veins in your esophagus and stomach. They aren't built for high pressure. When the pressure exceeds 12 mmHg, these thin-walled veins can rupture, leading to massive internal bleeding.
The goal of every treatment strategy is simple: lower that pressure and seal those leaks. The European Association for the Study of the Liver (EASL) guidelines emphasize a multidisciplinary approach. You don't just treat the bleed; you treat the underlying pressure. This involves a combination of drugs, endoscopic procedures, and sometimes complex interventional radiology techniques.
Endoscopic Band Ligation: The First Line of Defense
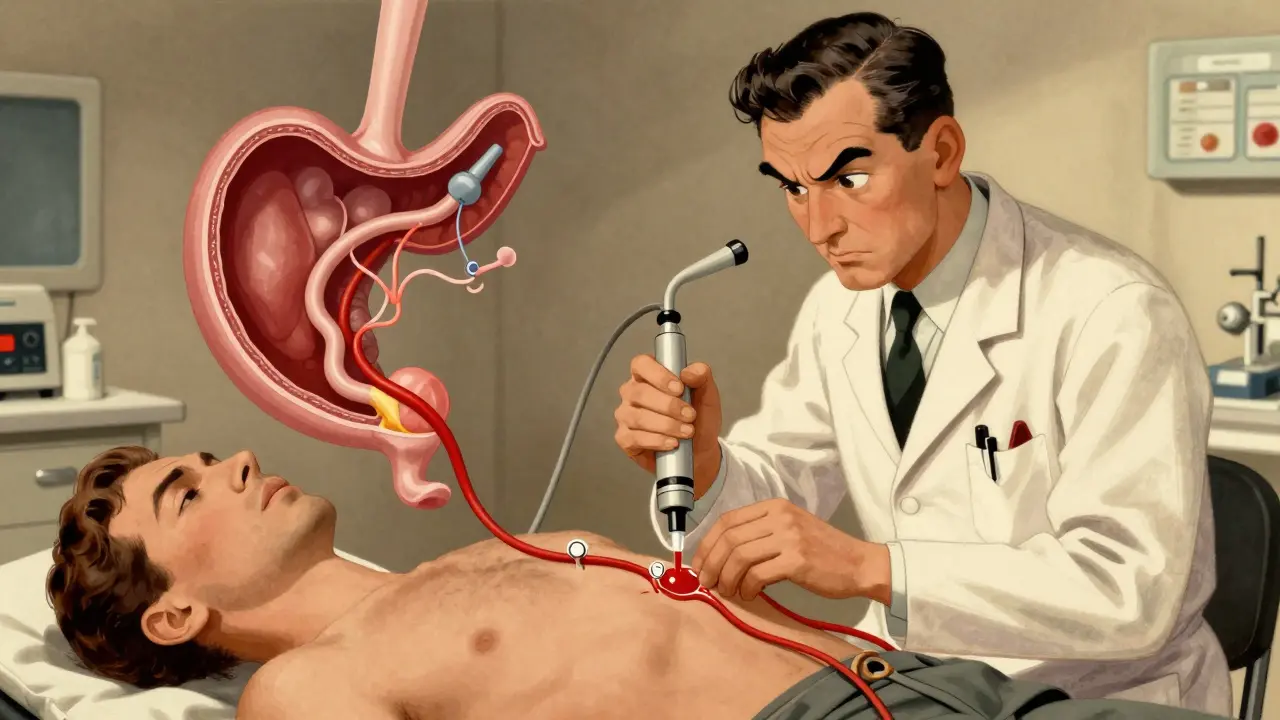
When a varix bleeds, seconds count. Endoscopic band ligation (EBL) is the gold standard procedure for stopping acute variceal bleeding and preventing recurrence. During this procedure, a gastroenterologist inserts a flexible tube with a camera (endoscope) down your throat. At the tip is a device that shoots small rubber bands around the swollen vein. The band cuts off blood supply to that section of the vein, causing it to clot, shrink, and eventually fall off like a scab. It sounds intense, but it’s incredibly effective.
- Speed is critical: Guidelines mandate performing EBL within 12 hours of presentation. Delays increase mortality risk significantly.
- High success rate: Initial hemostasis (stopping the bleed) succeeds in 90-95% of cases.
- Multiple sessions: One session rarely does it all. Most patients need 3-4 treatments spaced 1-2 weeks apart to completely eradicate the varices.
- Technology matters: Modern multi-band devices, like the Boston Scientific Six-Shot System, reduce procedure time by 35% compared to older single-band tools, making the process safer and faster.
While EBL is superior to older methods like sclerotherapy (injecting chemicals to scar the vein), it isn't perfect. If bleeding is so massive that the doctor can't see clearly, the procedure might fail. In those rare cases, alternative interventions become necessary. Also, some patients report sore throats or difficulty swallowing for a few days after banding, which is a normal part of the healing process.
Beta-Blockers: Lowering the Pressure Medically
You can’t rely on banding alone forever. To keep varices from growing back, you need to lower the overall pressure in the portal system. This is where Non-selective beta-blockers (NSBBs) come into play. These medications do two things: they slow your heart rate (reducing cardiac output) and constrict blood vessels in the gut (reducing splanchnic blood flow). Together, they drop portal pressure by 15-25%. The target is to get the hepatic venous pressure gradient (HVPG) down to ≤12 mmHg or reduce it by at least 20% from baseline.
There are two main players in this category:
- Propranolol: Often the first choice due to low cost. Starting doses are usually 20mg twice daily, titrated up to 160mg/day as tolerated. Generic versions cost just $4-$10 per month in the US.
- Carvedilol: A newer option that combines beta-blocking with alpha-blocking effects. Studies show it reduces portal pressure more effectively (22% vs 15% for propranolol). It starts at 6.25mg daily, titrating to 12.5mg. However, branded versions can cost $25-$40 monthly.
Despite their effectiveness, about 25-30% of patients struggle to tolerate therapeutic doses. Side effects like fatigue, dizziness, and low blood pressure are common. If you have asthma, severe bradycardia (slow heart rate), or decompensated heart failure, beta-blockers might be contraindicated for you. Always monitor your response closely with your hepatologist.
| Treatment Modality | Mechanism of Action | Success/Efficacy Rate | Key Limitations/Side Effects |
|---|---|---|---|
| Endoscopic Band Ligation | Mechanical strangulation of varix | 90-95% initial hemostasis | Requires multiple sessions; post-procedure pain |
| Propranolol | Reduces cardiac output & splanchnic flow | ~50% reduction in rebleeding risk | Fatigue, hypotension, bronchospasm risk |
| Carvedilol | Beta + Alpha blockade | Superior pressure reduction (22%) | Higher cost, similar side effect profile |
| TIPS Procedure | Surgical shunt bypassing liver | 86% 1-year survival in high-risk | 30% risk of hepatic encephalopathy |
When Standard Care Isn't Enough: TIPS and Beyond
Sometimes, despite banding and beta-blockers, the bleeding continues or recurs. For high-risk patients-specifically those with Child-Pugh B cirrhosis with active bleeding or Child-Pugh C scores ≤13-doctors may recommend a Transjugular intrahepatic portosystemic shunt (TIPS). This is a major intervention where an interventional radiologist places a stent inside the liver to create a direct channel between the portal vein and the hepatic vein. This bypasses the blockage entirely, drastically lowering pressure.
TIPS is powerful but comes with trade-offs. While it improves short-term survival (86% at one year vs 61% for standard care), it carries a 30% risk of hepatic encephalopathy-a confusion-inducing buildup of toxins in the brain because blood bypasses the liver's filtering system. Not every hospital can perform TIPS; only about 45% of U.S. hospitals have teams capable of doing it within 24 hours. Because of this, timing and location matter immensely. Experts debate whether to use TIPS early (within 72 hours) for all high-risk patients or reserve it for failures. Your medical team will weigh your specific liver function against the risks of encephalopathy.
For gastric varices (veins in the stomach rather than the esophagus), banding is less effective. In these cases, Balloon-occluded retrograde transvenous obliteration (BRTO) is often preferred. Data shows 30-day mortality drops from 6.2% with banding to 2.8% with BRTO for gastric cases. Vasoactive drugs like terlipressin or octreotide are also used during acute episodes to temporarily constrict blood vessels while preparing for endoscopy. Newer long-acting formulations of octreotide are emerging to improve adherence, moving from daily injections to monthly shots.
Living with the Risk: Patient Experiences and Realities
Managing variceal bleeding isn't just about clinical protocols; it's about living with a chronic, serious condition. Patients often share mixed feelings about the treatments. On forums, many praise banding for its immediate life-saving impact, noting quick discharges after successful procedures. Others describe the psychological toll of recurring appointments, saying they dread the banding sessions even though they know it saves their life.
Medication tolerance is another huge hurdle. Many patients report that propranolol leaves them too tired to function, forcing switches to carvedilol or dose adjustments. Cost is also a factor, especially for those without robust insurance coverage. The disparity is stark: uninsured patients face a 35% higher mortality rate than insured ones. Access to specialized centers matters too. High-volume centers (>50 procedures annually) have 15% lower rebleeding rates than low-volume ones. If possible, seek care at a center with dedicated hepatology and interventional radiology teams.
Adherence to medication and follow-up schedules is non-negotiable. Only 62% of patients fully adhere to standard octreotide therapy, and only 55% reach target beta-blocker doses within three months. Small lapses can have big consequences. Regular monitoring of blood pressure, heart rate, and liver function tests helps doctors adjust your regimen before a crisis occurs.
Prevention Strategies and Future Outlook
Prevention is the ultimate goal. Primary prevention (before any bleed) focuses on identifying high-risk varices via endoscopy and starting beta-blockers or banding early. Secondary prevention (after a bleed) combines both therapies indefinitely. Lifestyle changes support medical treatment: avoiding alcohol completely, managing salt intake to reduce fluid retention, and treating underlying hepatitis with antivirals if applicable.
The future looks promising. Artificial intelligence is being tested to predict bleeding risks earlier. New pharmacotherapies aim to reduce side effects. Trials like PORTAS are exploring ways to make TIPS more accessible. With integrated care, experts believe we could cut variceal bleeding mortality by 40% in the next decade. Until then, staying informed, adhering to treatment, and maintaining open communication with your healthcare team are your best defenses.
How quickly must endoscopic band ligation be performed after bleeding starts?
Current AASLD guidelines mandate that endoscopic band ligation should be performed within 12 hours of presentation. Delaying beyond this window significantly increases the risk of treatment failure and mortality.
What is the difference between propranolol and carvedilol for variceal bleeding?
Both are non-selective beta-blockers, but carvedilol also has alpha-blocking properties, allowing it to reduce portal pressure more effectively (22% vs 15%). Carvedilol is often more expensive and may cause more dizziness, while propranolol is cheaper and widely available as a generic.
When is a TIPS procedure recommended over banding and medication?
TIPS is typically reserved for high-risk patients who fail standard therapy or present with severe bleeding. Specifically, it is recommended for patients with Child-Pugh B cirrhosis with active bleeding or Child-Pugh C scores ≤13, where it significantly improves short-term survival despite the risk of hepatic encephalopathy.
Can variceal bleeding be prevented entirely?
While no method guarantees 100% prevention, combining endoscopic band ligation with non-selective beta-blockers reduces rebleeding risk by approximately 50%. Strict adherence to medication, regular endoscopic surveillance, and managing underlying liver disease are crucial for long-term prevention.
What are the common side effects of beta-blockers in liver patients?
Common side effects include fatigue, dizziness, low blood pressure, and slowed heart rate. About 25-30% of patients cannot tolerate therapeutic doses. Contraindications include asthma, severe bradycardia, and decompensated heart failure.



Comments
I find this breakdown of variceal bleeding protocols to be exceptionally thorough and well-structured. The distinction between primary and secondary prevention strategies is particularly illuminating for those of us who may not have a clinical background but wish to understand the nuances of hepatology care. It is encouraging to see such clear guidelines regarding the timing of endoscopic band ligation, as delays can indeed prove fatal in these acute scenarios.
Thanks for sharing this info. My dad has liver issues so I was looking into beta blockers. This helps me get it.
Great post! I wanted to add that while carvedilol is more effective at lowering pressure, many patients still prefer propranolol due to cost. In my experience working with patients, the financial burden often dictates the choice of medication more than the slight efficacy difference. Also, remember that TIPS isn't just for failures anymore; early TIPS is becoming standard for high-risk Child-Pugh B/C patients. It's a game changer if you can access it quickly. Hope this adds some value to the discussion!
It is fascinating how medicine has evolved from simply treating the symptom to managing the underlying hemodynamics. We used to think of varices as isolated events, but now we see them as part of a broader systemic failure. The optimism surrounding AI predictions for bleeding risk gives me hope that we will soon move towards truly personalized preventive care rather than one-size-fits-all protocols. Progress is slow but steady.
This is such an important topic!! 🌟 I’ve been researching this for my aunt who recently had her first bleed. The part about adherence really hit home because she struggles with taking meds regularly. It’s scary to think that missing doses could lead to another crisis 😱 But knowing that banding has a 90%+ success rate is super reassuring! Let’s keep spreading awareness so people don’t ignore their symptoms! 💪❤️
hey i read somewhere that diet plays a huge role too? like salt intake right? does anyone know if there are specific foods to avoid besides alcohol? im trying to help my brother out and he loves salty snacks lol. any tips would be great thx!
boring medical stuff. skip it.
The comparison table provided here is very useful for understanding the trade-offs between different treatment modalities. As someone who works in healthcare administration, I often see patients delayed in accessing specialized centers due to logistical barriers. It is crucial that we advocate for better distribution of interventional radiology teams, especially since only 45% of US hospitals can perform TIPS within 24 hours. Access is equity in this context.
OMG this gave me chills reading about the mortality rates! 😱 Its so scary how fast things can go wrong. I had a friend who ignored his fatigue and ended up in the ICU. Please listen to your doctors!!! Beta blockers are no joke but they save lives. Dont let the side effects scare you off without talking to your doc first. You got this! 💖
You need to stop ignoring your health or you will die. Its that simple. Take the pills. Go to the doctor. Stop complaining about tiredness and do what saves your life. No excuses.
the idea of pressure building silently is quite poetic in a dark way. we live with so much unseen tension until it bursts. maybe thats why liver disease feels so sudden even though its been brewing for years. interesting perspective on the mechanics of the body failing us gradually then all at once
I must commend the author for presenting such a comprehensive overview of current clinical guidelines. The emphasis on multidisciplinary care is paramount, as isolated interventions rarely yield sustainable outcomes in complex hepatological conditions. Furthermore, the statistical data regarding hospital volume and rebleeding rates underscores the necessity of centralized care models for optimal patient survival.
lol u guys take this so seriously. its just veins. :P