You look up at the bright sky or glance at a white wall, and suddenly, there they are-tiny specks, cobwebs, or worms drifting across your vision. You turn your eyes left; they drift right. You try to ignore them, but they seem to multiply. If you’ve experienced this, you’re not alone. These visual disturbances, known as eye floaters, along with sudden bursts of light called flashes, are incredibly common. For most people, they are harmless signs of aging. But for others, they can be the first warning signal of a serious condition that threatens permanent vision loss.
The difference between "normal" aging and an emergency often comes down to timing and pattern. Understanding what is happening inside your eye-the gel-like substance filling the space behind your lens-can help you decide whether to relax or rush to an ophthalmologist. This guide breaks down the science of vitreous changes, helps you identify dangerous symptoms, and tells you exactly when to seek care.
What Is Happening Inside Your Eye?
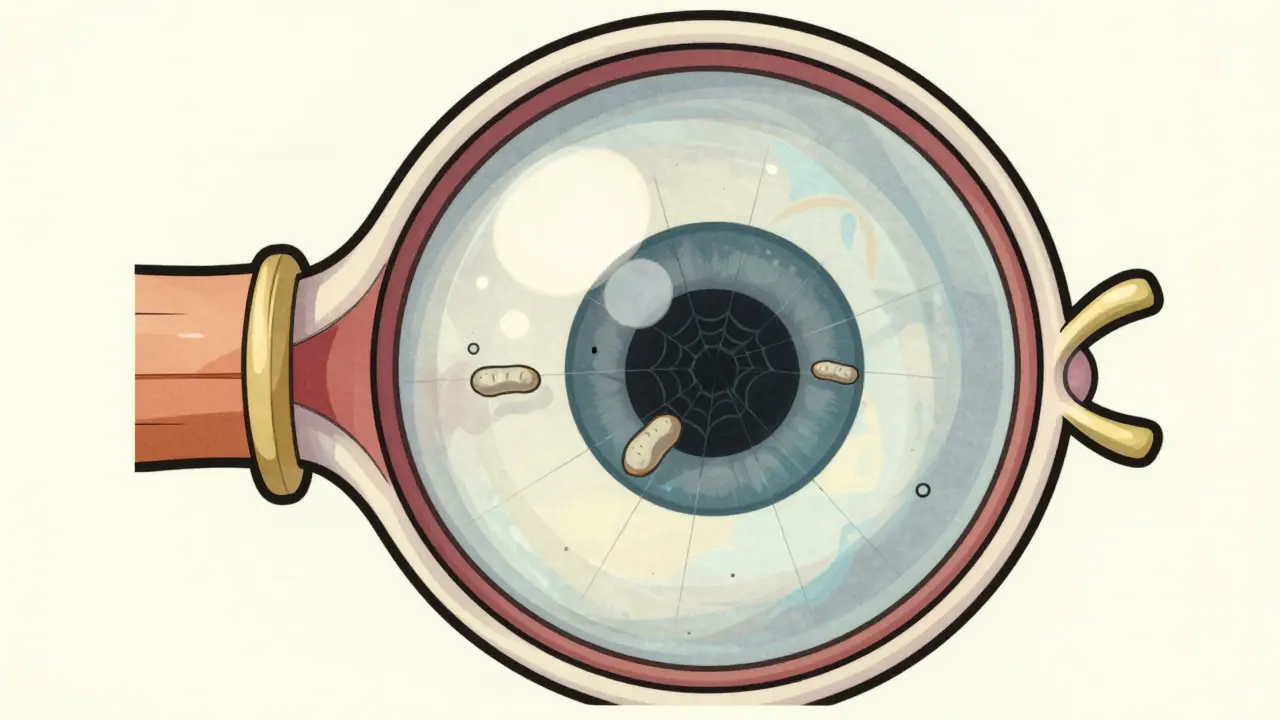
To understand floaters and flashes, you first need to understand the structure of the eye. The back two-thirds of your eyeball is filled with a clear, jelly-like substance called the vitreous humor. The vitreous humor is a transparent gel composed of 99% water and 1% collagen fibers arranged in a lattice structure that maintains the eye's shape and keeps the retina pressed against the back of the eye..
When you are young, this gel is firm and clear. However, as we age, typically starting around our 40s or 50s, this structure begins to break down. The collagen fibers clump together, and the gel starts to liquefy. This process is medically known as vitreous syneresis. As the gel shrinks and pulls away from the retina (the light-sensitive layer at the back of the eye), it creates the conditions for both floaters and flashes.
Think of the vitreous like a block of ice melting in a glass. As it melts, bubbles form and rise. In your eye, these "bubbles" are clumps of collagen casting shadows on your retina. That shadow is what you see as a floater. Because the vitreous is still attached to the retina in some spots, when it pulls away, it tugs on the nerve tissue. The brain interprets this mechanical tug as a flash of light, even if no actual light entered the eye.
Decoding Floaters: Shadows in Your Vision
Floaters appear because something is physically blocking or bending light before it hits your retina. They are not images projected by the outside world; they are internal artifacts. Here is how they typically present:
- Appearance: They can look like tiny black dots, gray specks, threads, cobwebs, or even worm-like shapes.
- Movement: They move with your eye movement. When you stop moving your eyes, you might notice them slowly drifting or settling downward due to gravity.
- Visibility: They are most noticeable against high-contrast backgrounds, such as a blue sky, a white computer screen, or a blank wall.
In many cases, these are simply microscopic debris floating in the liquefied vitreous. The National Center for Biotechnology Information (NCBI) notes that these are often just age-related changes where collagen fibers have broken and clumped. For the majority of people, especially those over 65, floaters are benign. About 75% of individuals over the age of 65 experience them. The brain eventually learns to filter them out, a process called neural adaptation, which usually takes about six months.
However, not all floaters are created equal. A single, large floater that looks like a ring or a cobweb might indicate a posterior vitreous detachment (PVD). PVD occurs when the vitreous completely separates from the macula (the center of the retina). While PVD itself is usually harmless, the separation process can sometimes pull too hard on the retina.
Understanding Flashes: The Warning Signal
If floaters are annoying, flashes are alarming. Medically referred to as photopsias, flashes appear as brief streaks, flickers, or sparks of light, usually in your peripheral (side) vision. They often look like lightning bolts or camera flashes.
Flashes happen because the shrinking vitreous is physically pulling on the retina. The retina contains photoreceptor cells that detect light. When these cells are mechanically stimulated by traction (pulling), they send a signal to the brain that mimics the sensation of seeing light. This is why you might see flashes even in a dark room.
The key characteristic of concerning flashes is their recurrence. Occasional, random flashes might be less urgent, but repeated flashes occurring within seconds or hours of each other are a major red flag. According to clinical guidelines from Duke Health, recurrent flashes signal potential retinal tears. The retina is delicate; if the vitreous pulls hard enough, it can tear the retinal tissue.

The Danger Zone: Retinal Tears and Detachment
This is where the situation shifts from "nuisance" to "emergency." The primary risk associated with vitreous changes is damage to the retina. There are two main complications to watch for:
- Retinal Tear: When the vitreous pulls away, it may snag on a spot where it is firmly attached to the retina. This creates a tear. Fluid from the vitreous can then seep through this tear.
- Retinal Detachment: Once fluid gets under the retina, it lifts the retina away from the back wall of the eye, much like wallpaper peeling off a damp wall. If left untreated, the detached retina loses its blood supply and dies, leading to permanent blindness in that eye.
The Royal Australian College of General Practitioners (RACGP) highlights that while Posterior Vitreous Detachment (PVD) affects about 66% of people over 70, the risk of complications varies. PVD alone has a relatively low complication rate (10-15%). However, if the PVD is accompanied by vitreous hemorrhage (bleeding into the eye), the risk of a retinal tear jumps to approximately 70%. This bleeding often presents as a sudden shower of hundreds of tiny black or red spots.
When to Seek Immediate Care: The Red Flags
Knowing when to call your doctor is critical. You cannot diagnose a retinal tear at home. Only a dilated eye exam by an ophthalmologist or optometrist can confirm the health of your retina. Here are the specific scenarios that require immediate attention:
| Symptom | Typical/Benign | Emergency/Urgent |
|---|---|---|
| Floaters | Few, stable, long-standing specks | Sudden onset of many new floaters |
| Flashes | Rare, occasional, only in extreme darkness | Recurrent flashes in peripheral vision, day or night |
| Vision Loss | None | Curtain-like shadow over part of vision |
| Color | Normal | Gray or black spots obscuring vision |
If you experience any of the following, do not wait. Seek same-day evaluation:
- A sudden increase in floaters: Especially if they look like a swarm of insects or dust particles.
- Persistent flashing lights: Particularly if they occur repeatedly in your side vision.
- A shadow or curtain: Any gray area or "curtain" appearing in your peripheral vision is a sign of detachment.
- Blurred vision: Sudden blurriness that doesn’t go away after blinking.
The Cleveland Clinic emphasizes that time is tissue. Retinal detachments are medical emergencies. Early detection and treatment can prevent vision loss in 90% of cases. If you suspect a detachment, every hour counts.
Who Is at Higher Risk?
While anyone can develop floaters and flashes, certain groups face higher risks for complications. Understanding your risk profile can help you stay vigilant.
- Age: The risk increases significantly after age 50. By age 70, most people will have experienced some degree of vitreous degeneration.
- Nearsightedness (Myopia): People with myopia have longer eyeballs. This stretches the retina thinner and increases the likelihood of vitreoretinal traction. Myopic individuals often develop PVD 10-15 years earlier than those with normal vision.
- Diabetes: Diabetic retinopathy can cause fragile blood vessels in the retina to leak or bleed into the vitreous, causing sudden floaters.
- Previous Eye Surgery or Trauma: Cataract surgery, laser eye surgery, or physical injury to the eye can accelerate vitreous changes.
- Family History: If close relatives have had retinal detachments, you may be genetically predisposed to weaker retinal tissue.
Diagnosis and Treatment Options
If you visit an eye care professional for new floaters or flashes, they will perform a comprehensive dilated eye exam. Drops are used to widen your pupils, allowing the doctor to see the entire retina, including the far periphery. They will look for tears, holes, or areas of weakness.
If the retina is healthy: No treatment is needed for benign floaters. Doctors recommend observation. Over time, the floaters may sink out of your line of sight, or your brain will learn to ignore them. Some patients find relief by moving their eyes up and down to shift the vitreous fluid temporarily.
If a retinal tear is found: It can often be sealed quickly using laser therapy or cryotherapy (freezing). This creates scar tissue that fuses the retina to the underlying wall, preventing fluid from getting underneath and causing a detachment.
If a detachment has occurred: Surgical intervention is required. Procedures may include pneumatic retinopexy (injecting a gas bubble to push the retina back), scleral buckle (suturing a band around the eye), or vitrectomy (removing the vitreous gel and replacing it with a saline solution or gas bubble).
Note on Laser Vitreolysis: Some clinics offer YAG laser treatment to vaporize floaters. However, this procedure remains controversial. Major organizations like the American Society of Retina Specialists note limited evidence for its efficacy and potential risks. It is generally not recommended for typical age-related floaters unless they are severely impairing quality of life and other options are exhausted.
Living With Floaters: Coping Strategies
For those diagnosed with benign floaters, the journey is one of patience. It can be frustrating to have debris in your vision, but anxiety often makes the perception worse. Here are practical tips to manage them:
- Adjust Lighting: Since floaters are visible against bright backgrounds, reducing glare with sunglasses outdoors or adjusting screen brightness indoors can help.
- Eye Movement: Gently moving your eyes up and down can displace floaters out of your central field of view.
- Stay Hydrated: While hydration doesn't cure floaters, maintaining overall eye health supports the ocular environment.
- Give It Time: Remember the six-month rule. Most patients report significant improvement as the brain adapts and the debris settles.
How quickly should I see a doctor for new floaters?
If you experience a sudden onset of many new floaters, especially accompanied by flashes, you should seek evaluation within 24 to 48 hours. If you also notice a curtain-like shadow in your vision, seek emergency care immediately, as this indicates a retinal detachment.
Are eye floaters always a sign of aging?
In adults over 50, yes, they are usually related to age-related vitreous changes. However, in younger people, floaters can be caused by inflammation (uveitis), bleeding from diabetes, or trauma. Therefore, any new floater warrants a professional check-up regardless of age.
Can eye exercises get rid of floaters?
No, there are no proven eye exercises that eliminate floaters. Moving your eyes may temporarily shift them out of your direct line of sight, but it does not remove the collagen clumps causing the shadows. The most effective "treatment" is time, allowing the brain to adapt.
Why do flashes happen only in one eye?
Vitreous degeneration and posterior vitreous detachment often occur asynchronously, meaning one eye ages differently than the other. Flashes are caused by traction on the retina in a specific eye, so you will typically perceive them only in the affected eye. Covering one eye at a time can help you determine which eye is experiencing the symptoms.
Is laser surgery safe for removing floaters?
Laser vitreolysis is considered experimental by many major retina specialists due to inconsistent results and potential risks, such as damaging the retina or increasing intraocular pressure. It is generally reserved for severe cases where floaters significantly impair daily life and other treatments are not viable. Consult a retina specialist for a personalized risk-benefit analysis.



Comments
I honestly feel like you are invading my personal space just by talking about this but I guess it is important to know. My eyes have been doing weird things lately and I feel so drained thinking about it. The way the vitreous shrinks sounds like a metaphor for my own life actually. It is just crumbling away bit by bit while I try to hold onto everything else. I need someone to tell me it is going to be okay because the anxiety is eating me alive right now.
floaters are just collagen clumps casting shadows on your retina its basic optics really people overcomplicate it all the time. if you see flashes its traction on the photoreceptors sending false signals to the brain. most of the time its benign posterior vitreous detachment which happens to almost everyone eventually. stop panicking and let your brain adapt via neural adaptation usually takes six months or so.
There is something profoundly unsettling about realizing that the very substance maintaining the shape of our eye is slowly turning into liquid, much like ice melting in a glass. It forces us to confront the impermanence of our physical form in such an intimate way. We spend so much time looking outward at the world, yet these internal artifacts remind us that we are always carrying our own debris within us. The cobwebs and worms drifting across our vision are not just biological noise; they are silent witnesses to the passage of time. Perhaps there is wisdom in learning to ignore them, to let the brain filter out the distractions until only the essential remains. It is a strange kind of meditation imposed upon us by biology itself.
Hey there! Just wanted to say that you are not alone in this experience. It is super common especially as we get older. Try not to stress too much about it. Most of the time it is totally harmless. If you are worried though definitely check with a doc. Hang in there!
i had this happen last year and it was scary af but turns out it was nothing serious. just keep moving ur eyes around and maybe drink more water lol. dont freak out unless u see a curtain coming down then go to the hospital fast. otherwise just chill and wait for ur brain to ignore them.
It is imperative that one understands the distinction between benign physiological changes and pathological emergencies. The vitreous humor undergoes syneresis, a process wherein the gel liquefies and collagen fibers clump. This is a natural consequence of aging. However, failure to recognize the signs of retinal detachment can lead to catastrophic vision loss. One must remain vigilant and seek professional evaluation immediately upon observing sudden onset symptoms. Do not neglect your ocular health.
As someone who works in healthcare, I can confirm that the pathophysiology described here is accurate. The vitreous humor is primarily water and collagen, and its degeneration leads to posterior vitreous detachment. In our region, we often see patients presenting with photopsias due to retinal traction. It is crucial to educate the public about the red flags such as sudden showers of floaters or curtain-like shadows. Early intervention with laser therapy or cryotherapy can prevent full detachment. Stay informed and proactive about your eye health.
Great breakdown of the mechanics here. For those asking about treatment options, it is worth noting that YAG laser vitreolysis is still considered controversial by many specialists. The risks often outweigh the benefits for typical age-related floaters. Surgical interventions like vitrectomy are reserved for severe cases. Generally, observation and neural adaptation are the standard approaches. Always consult a retina specialist before considering any procedural interventions.
Oh my goodness, reading about the retina tearing away makes my heart race! It is like a dramatic thriller movie playing out inside your own head. The idea that a simple tug on the nerve tissue can create a flash of light is both terrifying and fascinating. We are so fragile, aren't we? One little pull and everything could come undone. But then again, the resilience of the human body is amazing too. We adapt. We survive. We learn to live with the cobwebs dancing in our vision. It is quite poetic in a dark sort of way.
It is truly disheartening to observe how casually people dismiss the potential severity of retinal issues when in fact the consequences of negligence are far more profound than mere inconvenience. The article rightly points out that time is tissue, yet individuals often delay seeking care due to ignorance or fear. This lack of diligence is morally questionable given the availability of effective treatments. One should not treat their vision with such indifference when the stakes involve permanent blindness. A thorough understanding of the risk factors is essential for responsible citizenship.
lol another article telling americans to worry about their eyes while the rest of the world is fine. typical propaganda. anyway yeah floaters suck but dont let the medical industrial complex scare you into unnecessary procedures. keep america great by ignoring fake news like this :)
so basically your eye is just a bag of jelly that goes bad over time huh? i mean thats kinda gross when u think about it. why do we even have this stuff if its just gonna turn into garbage floating around. feels like bad design tbh. but whatever i guess we gotta deal with it. hope nobody gets detached retina cause that sounds painful as hell.
Sure, let's all panic about every speck of dust in our vision. Groundbreaking stuff. I'm sure the millions of people with floaters are just thrilled to hear it's 'normal.' Thanks for the reassurance, I guess. Now I'll just sit here and stare at the sky waiting for the curtain to fall. Thrilling.
I would like to add that staying hydrated is indeed beneficial for overall eye health although it may not directly cure floaters. It is important to maintain a balanced diet rich in antioxidants as well. Regular eye exams are crucial for early detection of any abnormalities. Please do not hesitate to consult with your ophthalmologist if you have any concerns. Take care of yourselves :)
just ignore them after a while they go away mostly. mine did anyway. dont stress too much about it unless it gets really bad then go see a doctor. easy peasy.