Imagine walking into a movie theater. The lights dim, the screen glows, but everything looks like an impressionist painting smeared by rain. You squint, trying to force your eyes to focus, but the blur remains. This isn't just an inconvenience; it is a signal that your eye's optical system is out of alignment. For billions of people worldwide, this daily struggle stems from refractive errors, which are optical imperfections in the eye's ability to focus light precisely on the retina.
Refractive errors are not diseases in the traditional sense. They are structural mismatches between the length of your eye and its focusing power. When light enters your eye, it should hit the retina-the light-sensitive tissue at the back-like an arrow hitting the bullseye. If it misses, whether landing in front or behind, your vision blurs. Understanding these errors is the first step toward clear sight, whether you need simple glasses or advanced laser surgery.
Understanding the Three Main Refractive Errors
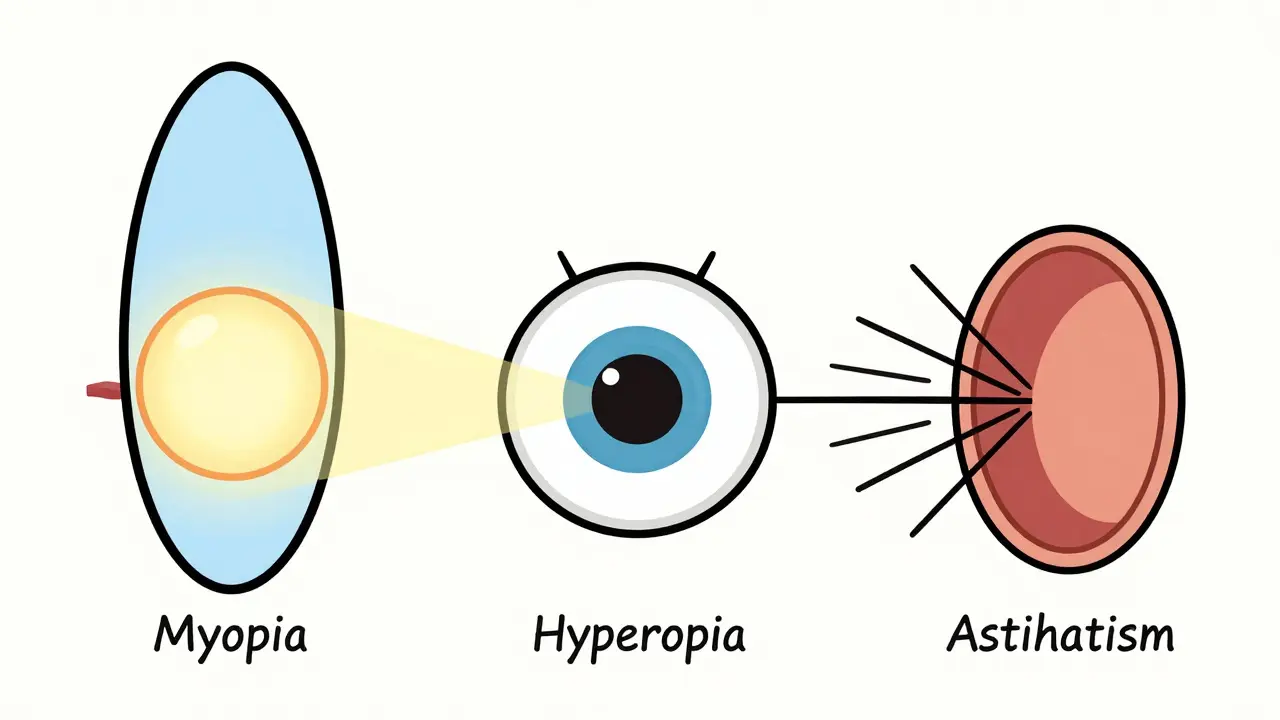
To fix the problem, you first have to identify which one you have. There are three primary types: myopia, hyperopia, and astigmatism. Each has a distinct cause and affects your vision differently.
Myopia, commonly known as nearsightedness, happens when your eyeball is too long or your cornea is too curved. In a normal eye, light focuses directly on the retina. In a myopic eye, that focal point lands in front of the retina. The result? Distant objects look fuzzy, while close-up tasks remain sharp. Myopia typically starts in childhood, around age 10, and progresses until late teens or early adulthood. It is incredibly common, affecting about 30% of the global population, with rates soaring to 80-90% among young adults in parts of East Asia.
Hyperopia, or farsightedness, is the opposite. Your eyeball is too short, or your cornea is too flat. Light rays converge behind the retina before they can form a clear image. People with mild hyperopia might see distant objects clearly because their eye muscles work overtime to compensate, but reading or doing close work causes significant strain, headaches, and fatigue. While often present at birth, symptoms usually become noticeable later in life as the eye’s natural lens loses flexibility.
Astigmatism is different from both. It doesn’t matter if your eye is too long or too short; the issue here is shape. Think of a basketball versus a football. A healthy cornea is round like a basketball. An astigmatic cornea is oval-shaped like a football. This irregular curvature causes light to scatter and focus on multiple points rather than one. Astigmatism can affect both near and distance vision simultaneously, leading to distorted images, glare, and difficulty driving at night. It affects roughly 30-60% of the population and often occurs alongside myopia or hyperopia.
| Condition | Anatomical Cause | Focus Point | Primary Symptom |
|---|---|---|---|
| Myopia (Nearsightedness) | Eye too long / Cornea too curved | In front of retina | Blurry distance vision |
| Hyperopia (Farsightedness) | Eye too short / Cornea too flat | Behind retina | Blurry near vision / Eye strain |
| Astigmatism | Irregular corneal shape (oval) | Multiple scattered points | Distorted/blurred vision at all distances |
Glasses and Contact Lenses: The Standard Corrections
The most immediate way to correct refractive errors is by bending light before it enters your eye. This is what glasses and contact lenses do. They act as external optics to compensate for your eye’s internal flaws.
If you have myopia, you need minus (-) power lenses. These lenses diverge light slightly before it hits your eye, pushing the focal point back onto the retina. If you have hyperopia, you need plus (+) power lenses that converge light, pulling the focal point forward. For astigmatism, standard spherical lenses won’t cut it. You need cylinder-shaped lenses with a specific axis orientation to counteract the irregular curvature of your cornea.
Glasses are safe, non-invasive, and offer instant clarity. However, they require consistent wear and can fog up, get wet, or fall off during sports. Contact lenses sit directly on the eye, offering a wider field of vision and better peripheral sight. But they come with risks. According to the CDC, about 3-4% of contact lens wearers develop microbial keratitis, a serious eye infection caused by poor hygiene or sleeping in lenses. Proper care is non-negotiable.
Refractive Surgery: Permanent Solutions
For many, wearing corrective lenses forever feels like a compromise. That’s where refractive surgery comes in. These procedures permanently reshape the cornea to change how light enters the eye. The goal is to eliminate the need for glasses or contacts entirely.
LASIK (Laser-Assisted In Situ Keratomileusis) is the most well-known option. Approved by the FDA in 1995, it uses a femtosecond laser to create a thin flap in the cornea, then an excimer laser to remove microscopic amounts of tissue. Modern lasers achieve precision within 0.25 diopters. Most patients experience immediate improvement in vision. However, it’s not risk-free. Dry eyes affect 20-40% of LASIK patients initially, and some report night vision issues like halos around lights.
PRK (Photorefractive Keratectomy) is similar but doesn’t involve creating a flap. Instead, the outer layer of the cornea is removed, and the underlying tissue is reshaped. PRK is often recommended for people with thinner corneas or those who participate in contact sports where a flap could be dislodged. Recovery takes longer, often several days to weeks for comfortable vision.
SMILE (Small Incision Lenticule Extraction) is the newer contender. It involves making a tiny incision and removing a small lens-shaped piece of tissue from inside the cornea. Because there’s no large flap, SMILE tends to cause fewer dry eye complications and offers faster structural stability. Projections suggest SMILE procedures will increase by 15% annually through 2028 due to these benefits.
To qualify for any of these surgeries, you generally need a stable prescription for at least 12 months, a corneal thickness of at least 500 microns, and must be over 18 years old. High myopia (greater than -6.00 diopters) carries higher risks, including a 5-10 times greater chance of retinal detachment, so thorough screening is essential.

Special Considerations for Children and High Myopia
Refractive errors aren’t just an adult problem. In fact, catching them early in children is crucial. The National Eye Institute notes that spending too little time outdoors and doing excessive close-up work are significant contributors to myopia development in kids. Left uncorrected, myopia can progress rapidly, leading to high myopia in adulthood.
High myopia is more than just needing strong glasses. It stretches the retina, increasing the risk of degeneration and detachment. To combat this, doctors are using innovative myopia control strategies. Orthokeratology (Ortho-K) involves wearing rigid gas-permeable contact lenses overnight to temporarily reshape the cornea. Studies show this can reduce myopia progression by 36-56%. Another emerging treatment is low-dose atropine eye drops (0.01%-0.05%), which have demonstrated a 50-80% reduction in myopia progression over two years in clinical trials.
Parents should ensure children get regular eye exams. Children often resist wearing glasses initially, but compliance improves significantly when they help choose the frames. Early intervention prevents long-term complications and supports proper visual development during critical learning years.
Living with Corrected Vision: Tips and Realities
Whether you choose glasses, contacts, or surgery, adjusting to corrected vision takes time. If you’ve never worn astigmatism correction, don’t expect perfection on day one. Users frequently report initial discomfort, with some noting it takes up to three weeks to adjust to new cylinder axes. Distorted vision, like looking through water, is common until your brain adapts to the new optical input.
For contact lens users, hygiene is paramount. Wash your hands before handling lenses, replace solution daily, and never sleep in them unless prescribed. For glasses wearers, invest in quality anti-reflective coatings to reduce glare, especially if you drive at night or work on computers all day.
If you opt for surgery, manage your expectations. While satisfaction scores are high (4.5/5 for LASIK based on aggregated reviews), perfect 20/20 vision isn’t guaranteed for everyone. Some may still need readers for presbyopia after age 40, regardless of prior surgery. Presbyopia is a natural aging process where the lens loses flexibility, distinct from refractive errors.
What is the difference between myopia and hyperopia?
Myopia (nearsightedness) occurs when the eye is too long, causing light to focus in front of the retina, resulting in blurry distance vision. Hyperopia (farsightedness) occurs when the eye is too short, causing light to focus behind the retina, leading to blurry near vision and eye strain.
Can astigmatism be cured with LASIK?
Yes, LASIK can effectively correct astigmatism by reshaping the irregular cornea into a more spherical shape. Wavefront-guided LASIK is particularly effective for complex astigmatism cases, mapping the eye's unique optical characteristics for precise correction.
Why do I need to wait 12 months for a stable prescription before surgery?
Refractive surgery reshapes your cornea based on your current prescription. If your prescription is still changing, the surgery will correct you for today's vision, but you may become nearsighted or farsighted again as your eyes continue to shift. Stability ensures long-lasting results.
Is Ortho-K safe for children?
Ortho-K is generally safe under professional supervision. It involves wearing rigid lenses overnight to temporarily flatten the cornea. It is particularly valued for slowing myopia progression in children, reducing the risk of developing high myopia and its associated retinal risks later in life.
What are the risks of contact lens wear?
The primary risk is infection, specifically microbial keratitis, which affects 3-4% of wearers. Risks increase with poor hygiene, sleeping in lenses, or exposing them to water. Regular check-ups and strict adherence to cleaning protocols minimize these dangers.